COVID-19 (originally published 11/2020)

Me testing my friend for COVID in the early days of the pandemic.
The COVID-19 event has been a disaster, but probably not in the way that you think.
Since the early days of it being identified, and starting to spread I have been trumpeting for a rational response (patting myself on the back here a little bit). I started posting on Instagram in March, with interpretations of papers and primary data.



My main hypothesis can be boiled down to:
COVID is not dangerous for people under 55
COVID very rarely spreads asymptomatically and pre-symptomatically
Both of these of these statements have strong scientific arguments. I would say they are true. The second argument is more difficult to argue, but I will attempt to do so.
COVID is not dangerous to people under 55:
This point has been more or less conceded by the media and mainstream science but I think it has been underplayed. I don’t need to spend much time on this argument, because it is a simple matter of fact.
In the US, 92% of deaths are people over 55, 58% of people are over 75.
This study is the largest estimate of the actual infection fatality ratio (IFR) of the virus, and puts the median estimate at 0.23%. (For reference, if that is correct than it is 2.3x more deadly than the seasonal flu.) If you aren’t familiar with the term IFR, it is basically a true estimate of how likely you are to die if you catch the virus. It also puts the median for people under 70 at 0.05%, about half of the flu. (From the WHO).

https://www.who.int/bulletin/online_first/BLT.20.265892.pdf
This following study works to delineate risk by age group, their overall IFR estimate is higher than the above study, most likely due to the population they are looking at. In serology studies on older populations, the IFR comes higher than 0.2, but in larger studies with a more representative sample it should approach the median. Regardless, the breakdown per age group should be close to accurate.
For people under 34, they estimate COVID is 7,000x less dangerous than someone over 85 (IFR of 0.004% vs. 28), or about 1,000x less dangerous than someone 75-85. This IFR is less than the seasonal flu for this demographic. For people up to 35-45 and 45-55 this rises to 0.068% and 0.23% in this study, which is not inconsequential but still a relatively low risk.
In the US group below 35 they estimate you are 3x more likely to die from an automobile accident (despite people 0-17 yr not driving). Think of how many times you have driven, and not died, divide that by 3 and that is your risk if you do catch COVID.
This study also notes that the rate of symptomatic infection is much lower in younger demographics. Studies demonstrating that schools are not a site of wide COVID spread corroborate this, and present some evidence for the next statement.

https://www.medrxiv.org/content/10.1101/2020.07.23.20160895v7.full.pdf+html
There has been some speculation about “long COVID” and people with mild cases suffering incomplete recoveries. At the moment I would say this is nonsense, to my knowledge (I looked) there have been no actual studies on this. There have only been anecdotes and doctors saying that it seems real. Without data it is fair to dismiss this.
COVID does not spread asymptomatically
As a scientist, this is a hot take. Nature has published a study suggesting that asymptomatic and pre-symptomatic spread makes up a high proportion of the spread. I am fairly certain that is not true.
In order for a respiratory virus to spread it must exit the body of an infected patient, and enter a healthy body. The gating step here is the exiting the body, you may have heard of droplets and aerosols.
The below study used an extremely sensitive technique to detect viral particles in the air. They measured the breath, and exhaled air in speaking, in several patients and found no detectable virus.


https://www.cambridge.org/core/journals/infection-control-and-hospital-epidemiology/article/escalating-infection-control-response-to-the-rapidly-evolving-epidemiology-of-the-coronavirus-disease-2019-covid19-due-to-sarscov2-in-hong-kong/52513ACC56587859F9C601DC747EB6EC
Study after study dances around the above fact. In order for there to be asymptomatic (or presymptomatic) spread the virus has to have some route out of the body. I guarantee if a study demonstrated that it would be published, and it is not. (The WHO agrees)

https://www.who.int/news-room/commentaries/detail/transmission-of-sars-cov-2-implications-for-infection-prevention-precautions.
You notice a common thread in every article or paper devised as proof of asymptomatic spread, that they never actually demonstrate particles of SARS-Cov2 in the breath or speaking or singing of asymptomatic patients, which would be required for them to pass the illness.
The physical “evidence” for it is all centered on weird physics modeling studies with fun 3d simulations, studies demonstrating it’s possible for influenza, demonstrating aerosols can be produced when singing, but never that COVID is detectable in these aerosols. These experiments would not require that much specialized equipment, so there is no reason that they would not already published if it were true.
The most cited paper on this comes from Nature, which was a modeling based study trying to determine serial interval time. It’s findings suggested that transmission often takes place before the development of symptoms, based on self-reported data. My immediate reaction to this is that it’s more likely that people tend to report getting symptoms later than they did out of shame of not isolating when symptoms became evident. It is telling that all the papers suggested as proof for asymptomatic spread are based on modeling of self reported data.
https://www.nature.com/articles/s41591-020-0869-5
One more commonly cited example of COVID aerosols comes from the New England Journal of Medicine. This one again, does not demonstrate COVID in aerosols of infected patients.
The study basically put the virus into a device that functions like a humidifier, and showed that it is possible to stay airborne. This is not relevant to humans, as most people are not putting COVID into humidifiers.
https://www.nejm.org/doi/full/10.1056/NEJMc2004973
You may remember the WHO saying they rarely see asymptomatic spread through contact tracing during the summer. (The article linked below is a perfect example of the cultural commentary that will follow this, with the source implying “we don’t actually have that answer yet” is about asymptomatic spread).
Some fuss was made about asymptomatic vs. presymptomatic. Regardless, I have not seen a convincing argument on how someone who is asymptomatic is different than someone who is genuinely presymptomatic. Both have similar levels of virus, and both do not have symptoms.

https://www.statnews.com/2020/06/09/who-comments-asymptomatic-spread-covid-19/
Further evidence can be seen looking at transmission within families (also known as secondary attack rate, SAR). This meta study estimated an 0.7% (1 in 140) chance that an asymptomatic person will pass COVID to a household member. To get a feel for what this means, flip a coin 7 times in a row. The odds of getting heads each time are about the same as passing covid to someone you live with when you are asymptomatic.

https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7402051/
You may be surprised to see that SAR for symptomatic cases to household members is only 20%. This is a topic for another essay, but it is has been seen in many studies. The field is starting to think that the bulk of spread happens in so-called superspreader events, where one symptomatic patient infects many people at the same time.
If both of my arguments are true, then lockdowns for people who do not have COVID symptoms, and are not in danger if they did get COVID, make very little sense.
Cultural Response and Lockdowns
The cultural response has been a travesty. The media has caused an immense amount of harm. Before COVID I had seen the New York Times as reliable, but in the early days of the pandemic it became very clear that they had no interest in truth. They have consistently fear-mongered, published deceptive articles, not corrected articles that were later shown to be false. I could write pages upon pages debunking their articles but I don’t have time. Almost everything they’ve published about COVID is misleading. This below article is a good example, at the time there had been fewer than 5 deaths in that age demographic. The asymptomatic spread article cites the same modeling studies commented on above, and some anecdotes that were later debunked as having a symptomatic person.
https://www.nytimes.com/2020/05/14/health/coronavirus-strokes.html
https://www.nytimes.com/2020/06/27/world/europe/coronavirus-spread-asymptomatic.html
The smears on Sweden are pretty revealing. Sweden is one of the only countries that did not lock down despite having substantial COVID in the population. Its mortality rates are often compared to other countries with younger populations, but looking at age adjusted mortality rates for all of these countries you can see that there has been virtually no change.

Further, comparing the deaths normalized to population, with current data, shows Sweden currently faring much better than the US and EU. Again, they never had lockdowns, mask mandates, or any business closures.

While the benefits of lockdown vs. an approach that allows for spread in non-vulnerable populations are dubious, the harm of lockdowns is clear.
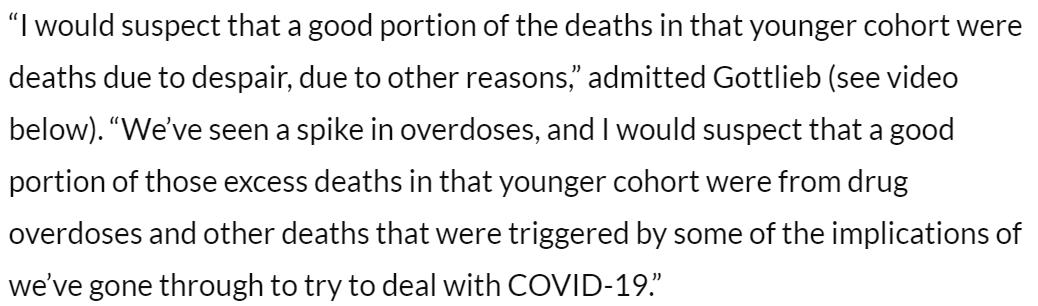
The knock on effects are causing rises in excess death in people not affected by COVID. Currently, in the US 1/3 of excess deaths are not COVID related. The largest rise in mortality by percent is men 25-44, which has no direct connection to COVID. There have been rises in heart related deaths, and there will no doubt be missed cancer screenings, and while the data is not out yet I suspect that suicide and overdose will be up this year. I personally lost a very close friend to suicide during the quarantine. This is corroborated by Scott Gotlieb, the FDA commissioner.
In order to tell the secondary effects it will be important to compare the non-COVID excess death to Sweden’s after this is all over.
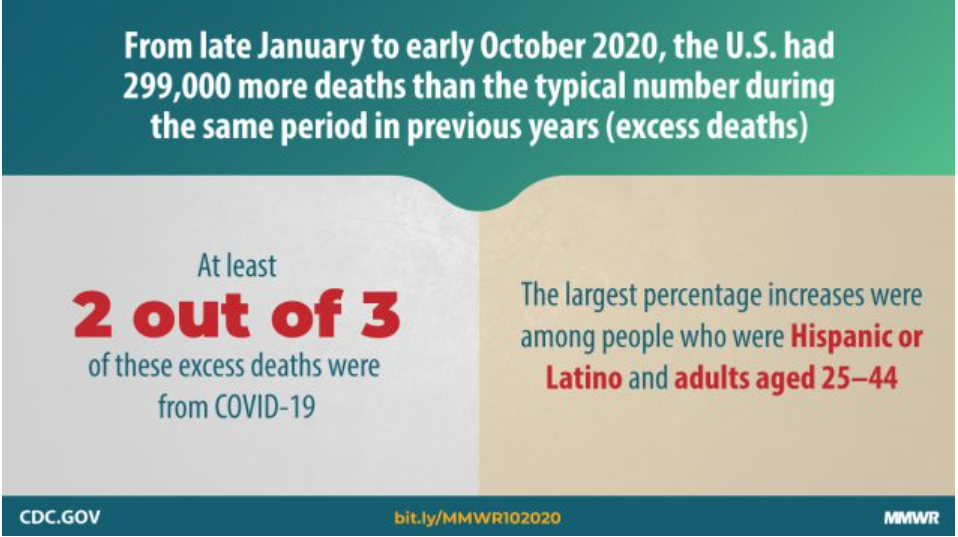
https://www.cdc.gov/mmwr/volumes/69/wr/mm6942e2.htm
In the developing world, the disruptions to supply chains for aid for have been clear. Poverty is increasing in developing nations for the first time in decades. For some sobering context read the below AP article.

https://apnews.com/article/lifestyle-ap-top-news-understanding-the-outbreak-hunger-international-news-5cbee9693c52728a3808f4e7b4965cbd
More troubling than the media is the response from the scientific community. The New England Journal of Medicine, Nature, JAMA, The Lancet, have all published work with extremely dubious conclusions. Generally the science in these big-name papers is decent, but the intro section and abstract present a narrative that fear-mongers. Because of the prestige of these journals, the media picks up the stories and they become a fact in the public mind.

This recent piece in the Lancet is a perfect example. Literally none of the highlighted statements are true.
For their claims about severity of infection they cite a paper with a sample size of 24 deaths, while there are papers with data for over 100,000.
They cite a Nature opinion piece with no data to support their claim of “Long COVID”.
They claim it is able to reinfect people, and cite a paper that documents the first and only confirmed re-infection, published in October. They fail to mention that durable antibody responses (7 months) have been demonstrated.
They later claim that herd immunity will never be reached.

https://www.eurekalert.org/pub_releases/2020-10/idmm-sad102320.php
The suggestion that we’ll never reach herd immunity, or herd immunity without vaccines is insanity. That is how virtually every pandemic that has ever happened has ended, relatively few have vaccines.
It is presented as the “evidence based” “scientific consensus”, and used to discredit scientists who rely on evidence. The term “listen to the scientists” has been thrown around in the media to silence dissent. It fails to acknowledge that scientists don’t all agree that lockdowns and masks are a good idea. Moreover it fails to acknowledge the culture of fear and homogeneity that is enforced by the “science” community. I know many scientists who are unwilling to publicly voice their opinions because of fear of repercussions from their university, or funding agency.
Cancellation is not too strong a word for what happens to scientists who dare to challenge the narratives. Nobel Prize winner Michael Levitt has been doing work to model the COVID outbreak. His work is widely recognized as being crucial in the foundation of bio-informatics. He is of the opinion that the lockdowns are harmful, and the virus has been overblown. He was recently dis-invited from giving a keynote address from a major conference, even though his presentation had nothing to do with his COVID research, because other speakers threatened to pull out if he was there.
Oxford epidemiologist Sunetra Gupta who authored the Great Barrington Declaration has been pulled from radio interviews and smeared by academics, dismissed as fringe, a liar. The Great Barrington is never mentioned without an attempt to tie it to right wing free market funding, or framing it as something akin to climate change denial. The lack of engagement on scientific ideas and resorts to personal attacks are absolutely shameful. Take this snip from a buzzfeed article.

I’m not sure what the media thinks they’ve uncovered with the link to the think tank, it doesn’t take a lot of funding to write up and publish a letter, and the "“medical and public health scientists” in quotes is just gratuitious. The critics mostly fail to mention that people advocating for this approach are people who have been studying epidemics for decades at Stanford, Harvard, Yale, Cambridge, Oxford, etc. There are experts on both sides.

In science discussion boards, making the case I made above has universally been met with responses guessing my political affiliations, calling me an idiot, linking to New York Times articles. I have been kicked out of a discord channel and a Facebook biology group personally (woe is me).
Current state of the world
Currently (11/11/20) case numbers are spiking around the world. For places that had a bad spring outbreak, the death numbers do not track the case numbers as they did in the first outbreak. This may be because of better treatments, but more likely it is because of widespread testing. We are simply running orders of magnitude more tests, and picking up a much higher percent of cases. In my opinion, picking up an asymptomatic case provides no useful information.
Places that did not have a high amount of COVID cases in the spring will suffer this winter, but without mass gatherings I suspect that transmission rates will still be lower. However, without having had the virus circulate through less vulnerable populations due to the lockdown, vulnerable populations will be equally exposed. The virus is absolutely dangerous for older people, and many may die. I would discount case number stories, and pay attention to death rates if you are interested in keeping up with the news.
A highly effective vaccine is likely less than a month away for emergency use authorization. Distribution and immunization of a high number of people will mark the end of the pandemic.
My guess is by the time it is manufactured and distributed to places that have had significant outbreaks (Jan-Feb 2021) they will have already hit herd immunity. New York has seen rising case numbers for weeks now, and does not have the tracking with death that was present in the first outbreak. This indicates fewer people are getting sick, and we’re simply identifying people who would not have been tested. If the death rate stays low into December, it would be fair to conclude NY has hit herd immunity.

http://levitt2.herokuapp.com/
I think the vaccine will do little more than provide an easy out to the institutions who got the whole thing so wrong. A pandemic that was woefully mishandled, and media institutions that have continuously lied to the public will be able to wash their hands of COVID without any accountability for the ordeal that the world will have gone through.
Please read and sign the Great Barrington Declaration
https://gbdeclaration.org/